Editor’s note: This article is one of the winners of the 2022 IDL SIG Student Outreach Article-writing Competition, and will be published in intercom‘s May/June 2022 issue. Congratulations, Edel!
The field of instructional design is rewarding if you have a passion for producing content for learners to succeed. Instructional design is the art of designing and iterating learning experiences and curricula to meet the learner’s needs. Continue reading “Becoming An Instructional Designer”
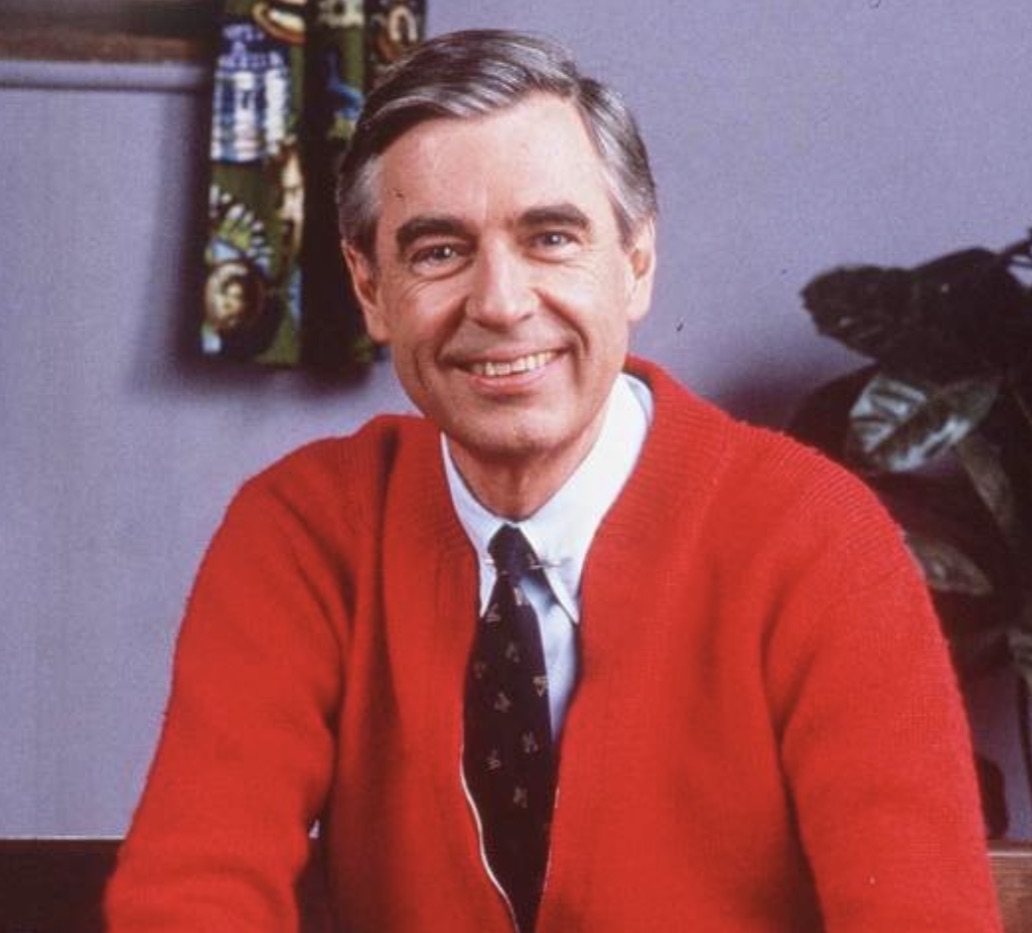
With an increasing demand for online learning, instructional designers are adapting existing online instruction programs to create remote learning. TV legends like Fred Rogers, LeVar Burton, and Bob Ross provided effective distance learning before it became widespread. What techniques do these three TV hosts offer instructional designers for effective workplace learning today?
Fred Rogers was more present virtually than most people manage to be in person.
Mister Rogers’ Neighborhood ran from 1968 to 2001, one of the longest-running children’s PBS series. Mr. Rogers spoke directly to children, validating their feelings and helping them name, face, and understand their emotions. Many have applied his methods to adult contexts such as leadership, HR, and pedagogy.
Mr. Rogers engaged children with open-ended questions, asking them about their experiences and urging them to draw upon prior knowledge. He presented models and examples in “The Land of Make Believe,” encouraging children to connect these to their own experiences. Jack Mezirow established transformative learning theory in 1978, with the concept that the learner’s critical self-reflection can transform the learner’s perspective (Mezirow, 2009). Mezirow grounded his concept in the foundational theory of constructivism, based on the idea that people actively create their knowledge and understanding. Your reality is determined by your experiences as a learner. Learner-centered instructionfurther acknowledges learners’ differences, shifting the planning and control of learning from the instructor to the learner.
Mr. Rogers exemplified this principle, to the extent one can on TV. While the children couldn’t direct the content on the episodes (the true learner-centered approach), his show included enough other content (such as visiting factories and interviewing guests) that the emotional instruction was an “offering” rather than a lesson to be imparted. Mr. Rogers’ gentle guidance and questioning put the learner at the center of the experience. He sang these words at the end of each episode: “I’ll be back, when the day is new, and I’ll have more ideas for you… You’ll have things you want to talk about… and I will, too.”
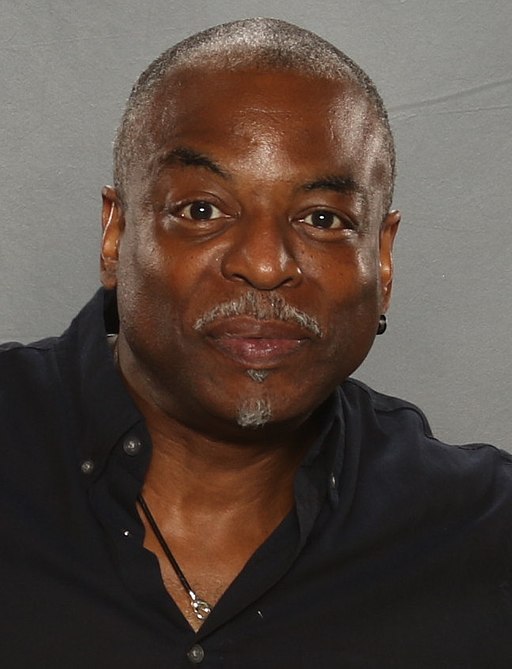
LeVar Burton helped a generation become self-directed learners.
Actor LeVar Burton (Roots, Star Trek the Next Generation) hosted Reading Rainbow on PBS from 1983 to 2009. This beloved show encouraged a love of reading by exploring various topics related to a featured children’s book. Segments approached books from many directions, from character interviews and celebrity appearances to visiting the book’s setting. Reading Rainbow earned over 200 broadcast awards, including a Peabody and 26 Emmy Awards. There are now interactive Reading Rainbow apps and video field trips for the iPad® and Kindle®.
LeVar taught around a subject, adding context by introducing related topics. Interdisciplinary learning combines learning objectives and methods from more than one branch of knowledge to focus on a central theme, issue, or problem. Interdisciplinary learning transfers knowledge gained in one discipline to another and deepens learning.
Even with LeVar’s acting skills, he didn’t read or dramatize the book. Learners were encouraged to read the books themselves. Sometimes people misunderstand self-directed learning (SDL)—it is not about working alone. SDL means a learner sets and often measures their own learning goals and progress. Another critical part of SDL includes sharing the learning process with peers and collaborating. LeVar would say, “But you don’t have to take my word for it…” Children would then come on screen and make book recommendations to each other.
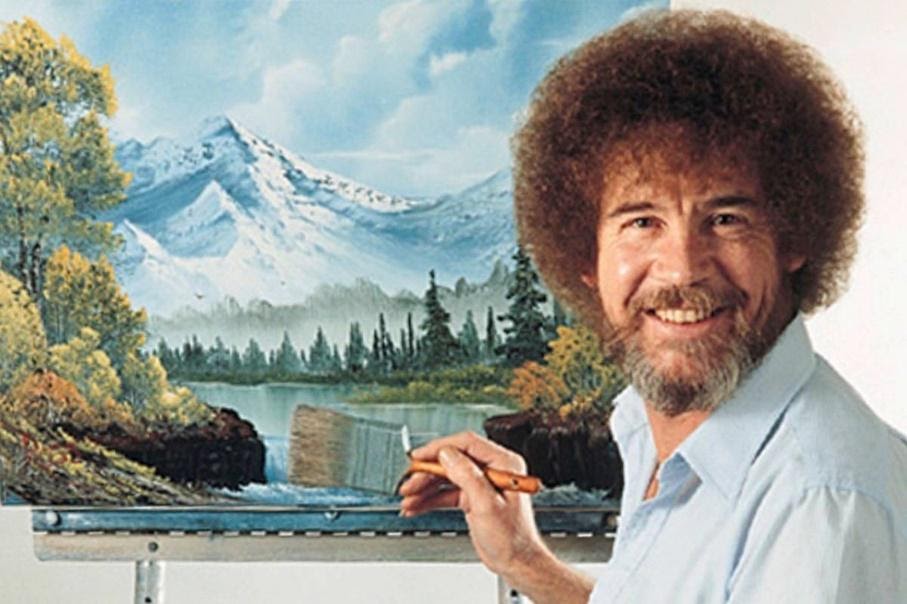
Bob Ross taught skills one happy cloud at a time.
Bob Ross hosted The Joy of Painting, another PBS television show that aired from 1983 to 1994. Bob Ross demonstrated with each brushstroke how to paint landscapes in oil. Many enjoyed watching him demonstrate specific landscape painting techniques by showing how to create integral elements, such as the sky, trees, and “happy clouds.”
Observational learning is a subset of social learning theory and describes learning from watching and mimicking others’ behaviors. Techniques of observational learning include modeling, shaping, and chaining. Observational learning is most common with children as they tend to copy adults naturally. However, on-the-job skills are also learned via observational learning.
People often develop new skills by shadowing. An example of this is having a new hire observe a more experienced employee on the job. Video tutorials and recorded screen captures are also observational learning.
Bob Ross’s consistency and demonstration of skills set his instruction apart. His impeccable planning of the show achieved this consistency. Bob planned each word and made three copies of his paintings for each show. Careful planning, prepping, and storyboarding are also vital to quality workplace learning and facilitation excellence.
Employ Learner-Centered techniques as Mr. Rogers did:
Build open-ended questions into the learning experience.
Have the learner draw upon their own experience and construct their own meaning.
Allow the learner to direct and take ownership of what is learned.
Encourage Self-Directed and Social Learning the same way as LeVar Burton:
Encourage independent exploration of content by providing ample resources and materials.
Build peer collaboration with discussion boards and communities of practices.
Use an interdisciplinary approach to teach many job functions around a single example.
Create consistent Observational Learning in the same way Bob Ross did:
Include demonstrations or simulations.
Provide guides to support workplace shadowing.
Prototype your learning assets.
Mr. Rogers’ listening and empathy were profound, allowing children to feel acknowledged without even being in the same room. LeVar Burton stimulated self-directed and social learning. Bob Ross led learners through excellence in observational learning. They engaged learners without being able to see or get feedback from them. You can use the same learner-centered, self-directed, social, and observational approaches employed by these famous TV educators to engage remote workplace learners today.
REFERENCES
Mezirow, Jack (2009). An overview on transformative learning. In Knud Illeris (ed.), Contemporary Theories of Learning: Learning Theorists — In Their Own Words. Routledge.
ACKNOWLEDGEMENTS
Photos of Fred Rogers and LeVar Burton were obtained from Wikimedia commons, who provide the sourcing and copyright information for them at the following links:
Instruction designers (ID) develop educational experiences. This task comes with the challenges of developing a product that is user friendly in a timely manner. Storyboarding is a tool that instructional designers use to deliver instructional designs and experiences through a linear sequence of images. These images visually predict and explore a user’s product experience. Storyboarding can aid to streamline the creation of instructional products. Ideally storyboarding is the solution for instructional designers to enhance their workload; however, that may not be the case. It is important to compare the benefits of storyboarding to the disadvantages, allowing instructional designers to determine if the process will benefit them.
Advantages of storyboarding in ID
Storyboarding is known to solve problems that instructional designers face in their everyday workload. The two main problems ID faces are:
Slow turn-around time.
Lack of guidance from subject matter experts (SME).
A solution for both of these problems lies within storyboarding.
Slow turn-around time
Instructional design involves two groups of people—IDs and SMEs. Both parties have very different jobs and are required to find common time to work on a project, causing difficulty in collaboration. This process becomes increasingly difficult when both parties come from different departments or companies. Traditionally, once an ID project has begun development, changes are difficult to make due to the nature of the project, causing an slower output when designers have to backtrack.
Storyboarding is a way to streamline a lengthy communication and development process by creating a visual representation of the learning process. This allows a SME to look at an instructional product and point out errors, and places in need of improvement. A storyboard structure will limit communication errors that will hinder the development process. It is easier to change content in a storyboard, than in an instructional product. Before finalizing a product, this is the most efficient way to work out any issues an instructional designer may face after development has begun.
Lack of guidance
Due to the communication issues instructional designers face with SMEs, there also is a lack of guidance on the content they are developing. Instructional design is a field where many of the developers on not well versed in the content they are creating. With that, their SMEs often don’t dedicate time for questions and clarification. Storyboarding can help with that process.
By creating a visual map of your instructions, it is easy to point out areas where you need clarification, or issues in the users learning process. By having this map, you can easily share where you need guidance with little explanation. This can also help the designer develop questions that will help the overall process before a meeting, to ensure there isn’t an overwhelming need for back and forth the SME may not have time for.
Constraints
With the advantages of storyboarding to develop ID there are also disadvantages to the process. As the solution solves major issues in the process it develops others.
The two main issues surrounding ID and storyboarding are:
Lack of software.
Linear output.
For storyboarding to work there are assumptions about the ID development process that may not be true.
Access to storyboarding software
For professional instructional designers a company will give them a set of tools needed to do their jobs correctly. Seldom will an organization feel it is beneficial to invest in storyboarding software and training to develop content. With that, there is no software dedicated specifically to ID. The designer would have to invest their own money in it, and use a program that is made for film. That step would cause further issues as one member of a team would be working separately. Unless storyboarding is a solution a company is invested in or the designer is freelance, the process will not work.
Linear output
Storyboarding is a linear process causing a linear output. This approach to learning can hinder the user’s experience. A concept may be best presented in a matrix fashion where learning points can be cross-referenced or taught parallel to one another, in order to enhance an understanding of concepts. The design is not always going from point A to point B.
Conclusion
Storyboarding can be a useful tool in the world of ID but it is not for everyone. If a designer is creating a learning process that is best developed in a linear fashion, while having access to the correct software, it can help the ID development process in a positive way. Creating a storyboard when it does not best fit the learning plan can cause issues in development and user interaction. It is up to the designer to research and determine what development practice is best for them to make the most impactful user experience.
Nicole is currently completing a Graduate Certificate in Technical Communications at Seneca College, after receiving an undergraduate degree at York University in Professional Writing. She is excited to transition into the field of Technical Communications. Outside of writing, she is interested in Art History and enjoys reading.
Perhaps the first thing that comes to mind when you think of simulations is the flight simulator, maybe something like the Link Trainer (pictured in Figure 1). Flight training is well suited to simulation, as it is potentially dangerous and involves expensive hardware. The medical profession shares – and surpasses – these risks, making it fertile ground for simulation-based education. From antiquity, medical simulation used clay, stone or wood mannequins to allow students to practice medical procedures safely, as described by Meller.
Figure 1: The Link Trainer, the first flight simulator, built in 1929.
Modern medical simulation still uses mannequins (though stone and clay have been replaced by silicone and circuitry) as well as virtual simulations. Most medical education institutions employ some form of both of these modalities of simulation as described by May. Multiple studies have demonstrated the effectiveness of simulation for medical education, such as those conducted by Underwood and McKinney. Fidelity refers to how closely a simulation resembles the real-world experience it aims to simulate. New materials and technology for mannequins have dramatically increased their fidelity in the last thirty years. Virtual reality is experiencing a similar boom in recent years as computer horsepower and rendering techniques come closer to matching the real operating room (OR).
To VR or not to VR
Developing training for medical professionals today means choosing an approach out of a large and varied toolbox. Virtual Reality (VR) is one of these tools and its appeal is only growing. VR is a cost-effective and versatile alternative to expensive mannequins or specialized trainers. The main barrier to VR replacing other simulation methods has long been fidelity, as described by Satava. However, fidelity seems to have a limited effect on learning outcomes as found by Yang. Isaranuwatchai evaluated the cost effectiveness of a series of training methodologies: VR, high fidelity mannequin and progressive (VR and mannequin). They found that, depending on the funds available for investment in training programs, VR provides good return on investment in terms of learning outcomes.
Just as medical training mannequins experienced a significant leap in fidelity in the 1990s with the improvement of materials available and computer hardware and software for information gathering and feedback as described by Meller and Cooper, VR is in the nascent stages of a similar revolution. Stronger computer hardware and rendering techniques, as well as commercially available, affordable VR hardware herald a new age for VR as described by Rothman. The technology exists for high-fidelity medical training simulations, but the investment does not. Even the most recent simulations lag behind video games for entertainment in fidelity by at least a decade.
A VR Simulation for Advanced Cardiac Life Support (ACLS) Training
Figure 2: A screenshot of Vankipuram and colleagues’ cardiac life support simulation (left) and an input device designed to simulate compressions (right).
Vankipuram and colleagues have taken a step toward closing this gap. They have developed a VR simulation for cardiac life support training using a modern game engine (UnrealEngine), VR headsets and customized input devices (see figure 2). Networking allows students to work together, each filling a role on the trauma team. A customized UI provides real-time feedback on performance, while detailed data is gathered for evaluation and debriefing by an instructor. One of the biggest advantages of VR simulations over their practical counterparts is their ability to record large amounts of detailed information. Traditional mannequin simulations rely on the instructor to observe and provide feedback on each team member’s individual performance, while VR simulations can record every detail of every action of each team member.
Remote Facilitation
Another benefit of VR simulations for medical training is the potential for remote facilitation. Availability of specialized facilitators can be a major impediment to effective medical instruction. Ohta and colleagues compared a remotely facilitated, VR simulation-based pediatric resuscitation training module for medical students with the same program facilitated locally. They found no significant difference in learning outcomes for the remote facilitator versus the local one. Remote facilitation has the potential to greatly improve access to high-quality instructors in specialized fields across institutions at lower cost and with greater flexibility than requiring an in-person facilitator.
Next Steps
This work is a step in the right direction, but greater investment in the development of high-fidelity VR simulations for medical training is needed. The role of fidelity in the effectiveness of medical simulations is disputed. Yang and colleagues found no correlation between fidelity and effectiveness, while Isaranuwatchai and colleagues found that high-fidelity mannequins provide some improvement to learning outcomes over low-fidelity VR simulations. As VR simulations improve, more research is required to compare their effectiveness with more traditional methods of instruction, especially high-fidelity mannequins.
Remote facilitation has long been touted as the future of education. With the advent of reliable, fast internet connections and high-fidelity VR and the sense of presence it provides, remote facilitation is becoming more feasible. The future of medical education is virtual.
References
Christensen, M., Tan, S., Rieger, K., Dieckmann, P., Oestergaard, D., & Watterson, L. (2013). A Comparison of the Relative Effectiveness of Remotely and Locally Facilitated Simulation-Based Training of Medical Emergencies by Postgraduate Healthcare Teams. Simulation in Healthcare: The Journal of the Society for Simulation in Healthcare,8(6), 526.
Cooper, J. B., & Taqueti, V. R. (2008). A brief history of the development of mannequin simulators for clinical education and training. Postgraduate Medical Journal,84(997), 563-570.
Underwood, L., Ginkel, C. V., Lee, D., Wong, M., Dizaiy, S., Fry-Bowers, E., Nguyen, H. (2008). 153: Effectiveness of Medical Simulation on Knowledge in Septic Shock Management During Pre- Clinical Medical Training. Annals of Emergency Medicine,51(4), 517.
Dotson, M. P., Gustafson, M. L., Tager, A., & Peterson, L. M. (2018). Air Medical Simulation Training: A Retrospective Review of Cost and Effectiveness. Air Medical Journal,37(2), 131-137.
Fletcher, J. D., & Wind, A. P. (2013). Cost Considerations in Using Simulations for Medical Training. Military Medicine,178(10S), 37-46.
Isaranuwatchai, W., Brydges, R., Carnahan, H., Backstein, D., & Dubrowski, A. (2013). Comparing the cost-effectiveness of simulation modalities: A case study of peripheral intravenous catheterization training. Advances in Health Sciences Education,19(2), 219-232.
Lin, W., & Song, Y. (2017). Effectiveness of different numbers of simulation training models on medical students’ cervical examination performance. International Journal of Gynecology & Obstetrics,141(2), 255-260.
Mckinney, J., Cook, D. A., Wood, D., & Hatala, R. (2012). Simulation-Based Training for Cardiac Auscultation Skills: Systematic Review and Meta-Analysis. Journal of General Internal Medicine,28(2), 283-291.
Meller, G. (1997). A typology of simulators for medical education. J Digit Imaging,10(3), 194-196.
Ohta, K., Kurosawa, H., Shiima, Y., Ikeyama, T., Scott, J., Hayes, S., Nishisaki, A. (2017). The Effectiveness of Remote Facilitation in Simulation-Based Pediatric Resuscitation Training for Medical Students. Pediatric Emergency Care,33(8), 564-569.
Rothman, J. (2018, April 2). Are We Already Living in Virtual Reality? The New Yorker.
Satava, R. (2013). Keynote speaker: Virtual reality: Current uses in medical simulation and future opportunities & medical technologies that VR can exploit in education and training. 2013 IEEE Virtual Reality (VR).
Vankipuram, A., Khanal, P., Ashby, A., Vankipuram, M., Gupta, A., Drummgurnee, D., Smith, M. (2014). Design and Development of a Virtual Reality Simulator for Advanced Cardiac Life Support Training. IEEE Journal of Biomedical and Health Informatics,18(4), 1478-1484.
Yang, C., Wang, H., Chou, E. H., & Ma, M. H. (2012). Fidelity does not necessarily result in effectiveness – A randomized controlled study in a simulation-based resuscitation training for medical students. Resuscitation,83.
Maxwell Delamere-Sanders is a student in the Seneca Technical Communication Certificate Program at Seneca College. He completed a degree in English and Psychology at the University of Toronto in 2016, and is excited to bring his passion for language and the human mind to bear on the field of technical communication.
Simulations in medical training are a realistic cross-disciplinary method of training and feedback. In simulation-based learning learners can repeatedly practice and review tasks in lifelike circumstances using physical or virtual reality models to identify and understand the factors that affect systems and the problems that can arise. Simulation-based medical education (SMBE) allows students the chance to refine their skills in a safe and controlled environment where they can increase their skills and reduce their margins of error. SMBE creates a safe and controlled environment that exposes trainees to dangerous conditions.
The State of Medical Education
Research by Jones, Passos-Neto and Braghiroli indicates that, despite advances in technology, teaching strategies and learning theories, it is not uncommon for medical students to be taught with decades-old syllabi. The current model of medical training has been in use for at least a hundred years, but a developing movement for patient safety has forced institutes to revise the medical education system.
Several external factors are driving the movement for medical education reform:
Increased awareness of information overload and stress on medical students.
Recognition of the need for students to be effective junior doctors after undergraduate studies, not during residency; students are often ill-prepared for their roles.
The need for continuing education for higher specialist training, coupled with the drive to revalidate.
New interest in outcomes-based education, focusing on the student’s ability to perform what they have learned, rather than the typical goal-based education, which focuses on student satisfaction.
Some institutions have already adopted simulations for use in examinations. For example, Scalese, Obeso and Issenberg indicate that the Royal College of Physicians and Surgeons in Canada uses simulations with computers and mannequins alongside patient participants in their Internal Medicine certification exams.
Simulations, Past and Present
Any person attempting to determine the origins of simulation-based education would find themselves mired in information dating back millennia. While the first dedicated use of simulations in medical training took place in the USA in the 1960s, use of simulations in medical training can be found across cultures and ancient civilizations. In the past, these simulations used active participants or mannequins as the test subject. Over the last several decades, the educational tools shifted from the real-world to the virtual.
A Shift toward the Virtual
Medical education is one of many disciplines experiencing a significant increase in the use of simulation technology for teaching and assessment. From the military and aviation industries training pilots on flight simulators to construction workers training on virtual cranes, simulation-based education has seen a boom in trust and satisfaction.
The shift to virtual education for medicine follows the trends of society. Many medical students and practitioners have adapted their methods to better fit the 21st century:
Many medical students view lectures online or listen via podcasts.
Residents consult information stored in Personal Digital Assistants (PDAs) to make patient management more efficient.
Practitioners can receive continuing education credits by attending teleconferences.
Much of the movement toward simulations occurred in the 1980s and 1990s, when sophisticated computers and software capable of reproducing and mimicking physiologic responses and feedback were produced. The first wave of simulated patients combined a Macintosh computer with a mannequin and waveform generator to mimic a patient during anaesthesia. Specialties such as anesthesiology, critical care and emergency medicine have long been at the forefront of the push toward SMBE.
Technological innovations have paved the way for a wide range of simulators that can facilitate and supplement learning in numerous medical disciplines.
The Limits of SMBE
Primary concerns regarding simulation use in medicine involve cost, efficiency and simulation quality.
Cost: The best medical simulations are available at considerable costs. Machines require maintenance and updating, which continually adds to the initial purchase price.
Efficiency: Incorporating time into current medical curriculums is problematic and would require the medical curriculum to be updated. Dedicated and exclusive resources are seldom available. For simulations, an instructor-to-learner ratio of 1:3 or 1:4 is ideal, where the current ratio is between 1:10 and 1:15.
Simulation Quality: Human systems are complicated and varied, thus models and instruments can never completely mimic each iteration. Poorly designed simulations can inhibit learning, such as causing students to neglect checking for physical signs because they are absent in the simulation. Participants will naturally approach simulations differently than they would real life. Students will either be hypervigilant or negligent.
Long-term studies must be conducted to analyse the effects of SMBE on patient care and general effectiveness as a teaching tool. It is only after the impact of SMBE has been evaluated that simulations can begin to replace all outdated teaching materials.
Where To, Next?
The current model of medical education has changed little over the last hundred years, but an increase in demand for experienced doctors has pushed educational institutions to reconsider the system. Simulation on its own cannot guarantee learning, but it is a game-changer.
Future studies should be conducted regarding the effects of SMBE on improving patient outcome. Without strong evidence, a field as costly and vital as medical education cannot be altered with any severity. At best, simulations will be a periphery in medical education and training. The potential growth for SMBE alongside technological advances is unmeasurable and may be the key to training medical professionals in the future. However, institutions and practitioners must analyse the current education system and the validity of SMBE research to determine if the jump can be made now or later.
The shift toward heavy technology use is unavoidable; medical professionals, as other professions, have started to rely on computer- and cloud-based materials to improve their patient care. What remains to be seen is if they will fully accept this paradigm shift and trust simulations to train the next generation of doctors.
Resources
Bradley, Paul. “The History of Simulation in Medical Education and Possible Future Directions.” Medical Education 40, no. 3 (March 2006): 254-62. doi:10.1111/j.1365-2929.2006.02394.x.
James, John T. “A New, Evidence-based Estimate of Patient Harms Associated with Hospital Care.” Journal of Patient Safety 9, no. 3 (September 2013): 122-28. doi:10.1097/PTS.0b013e3182948a69.
Jones, Felipe, Carlos Eduardo Passos-Neto, and Oddone Freitas Melro Braghiroli. “Simulation in Medical Education: Brief History and Methodology.” Principles and Practice of Clinical Research 1, no. 2 (July/August 2015): 56-63.
Krishnan, Divya G., Anukesh Vasu Keloth, and Shaikh Ubedulla. “Pros and Cons of Simulation in Medical Education: A Review.” International Journal of Medical and Health Research 3, no. 6 (June 2017): 84-87.
Scalese, Ross J., Vivian T. Obeso, and S. Barry Issenberg. “Simulation Technology for Skills Training and Competency Assessment in Medical Education.” Journal of General Internal Medicine 23, no. Suppl 1 (January 2008): 46-49. doi: 10.1007/s11606-007-0283-4.
Serena Zaccagnini is a student at Seneca College in Toronto, Ontario studying Technical Communication. She is looking forward to a career in the Technical Communication field. I have a Specialized Honours Bachelor of Arts in English and Professional Writing with emphasis on Digital and Institutional Communication from York University. In my spare time, I enjoy reading and baking.




{kind=link}
{kind=link}